Physical Address
8206 Louisiana Blvd NE, Suite A N03815
Albuquerque, NM 87113
United States
Physical Address
8206 Louisiana Blvd NE, Suite A N03815
Albuquerque, NM 87113
United States

Your knee hurts, your hip aches, or your hands are stiff every morning. Doctors throw terms around—osteoarthritis, rheumatoid arthritis, bursitis—but rarely explain what's actually happening inside your joints. Understanding your specific condition changes everything. Not just knowing the name, but truly understanding the mechanism, progression, and what actually helps. This guide breaks down the most common joint conditions in plain language.
Your knee hurts. Or your hip. Or your hands are stiff every morning. You’re wondering if it’s arthritis, which kind, whether it’ll get worse, and what you’re supposed to do about it.
Doctors throw terms around—osteoarthritis, rheumatoid arthritis, bursitis, tendonitis—but rarely take time to explain what’s actually happening inside your joints, why it happened to you, and what the diagnosis really means for your life.
I’ve spent years learning these conditions from every angle I could find—research papers, medical texts, but more importantly, from people actually living with them. Including myself and people close to me. What I’ve learned is that understanding your specific condition changes everything.
Not just intellectually knowing the name, but truly understanding the mechanism, the progression pattern, what influences it, and what your realistic options are. That knowledge shifts you from passive victim to active participant in managing your joint health.
Understanding joint conditions is only part of the equation — long-term outcomes depend on applying the core principles of joint health, including movement quality, muscle strength, nutrition, and recovery.
This guide breaks down the most common joint conditions in plain language. What’s actually happening at a tissue level, why it happens, how to recognize it, how doctors diagnose it, and most importantly, what actually helps versus what’s just noise.
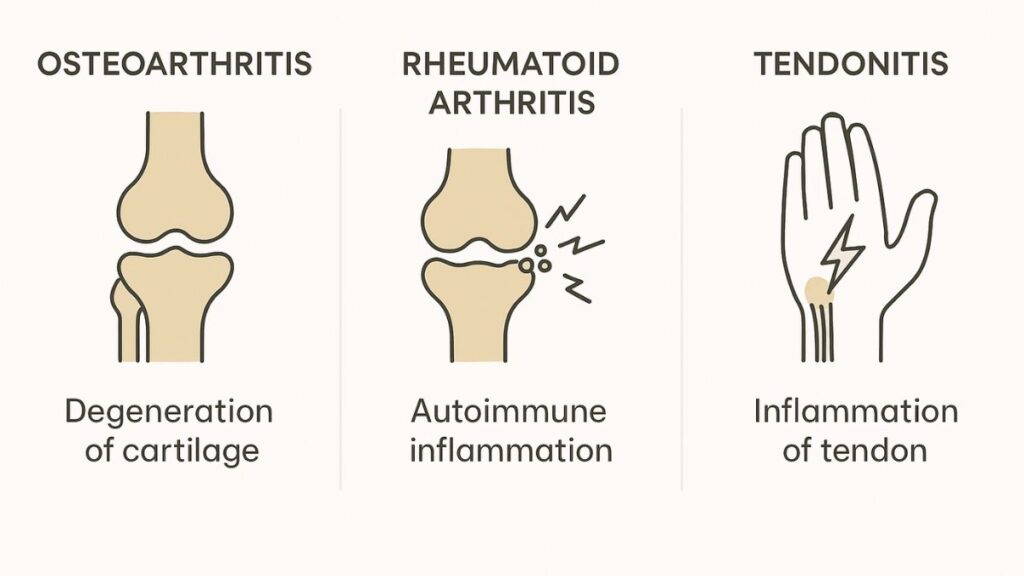
Osteoarthritis is the most common form of arthritis worldwide and a leading cause of disability among older adults. If your joints hurt and you’re over 50, this is probably what you’re dealing with.
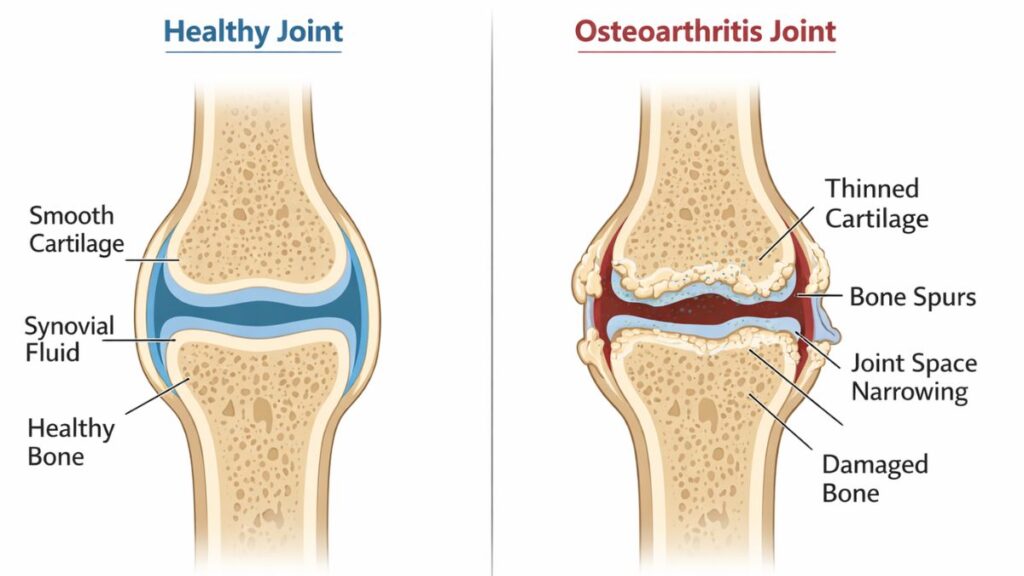
Osteoarthritis is fundamentally about cartilage breakdown. The smooth, slick tissue cushioning your joint surfaces gradually becomes rougher, thinner, and less effective. In advanced cases, it can wear away completely in areas, leaving bone rubbing on bone.
But it’s not just passive wear and tear like tires on a car. Your body actively responds to cartilage damage in ways that create additional problems. The underlying bone thickens and forms spurs (osteophytes). The synovial lining becomes inflamed, producing excess fluid. Ligaments may stretch. Muscles around the joint often weaken from disuse or altered movement patterns.
This is why OA isn't purely mechanical—there's an inflammatory component that matters. Low-grade chronic inflammation drives symptoms and accelerates cartilage loss. Managing that inflammation becomes crucial.
Multiple factors contribute, often simultaneously:
Mechanical stress patterns: Misalignments, previous injuries, repetitive movements, and abnormal loading create uneven stress on cartilage. The areas bearing extra load wear faster. This is why OA often develops asymmetrically—one knee worse than the other, specific parts of joints affected first.
Age: Cartilage becomes less resilient over time. Repair mechanisms slow. But age alone doesn’t cause OA—plenty of 80-year-olds have minimal arthritis. Age increases risk but doesn’t guarantee disease.
Weight: Every pound of body weight multiplies force on knees and hips with movement. Excess weight accelerates cartilage breakdown in weight-bearing joints. But it’s not just mechanical—fat tissue produces inflammatory compounds that contribute to joint degradation.
Genetics: Family history matters. Certain genetic variations affect cartilage composition and repair capacity. Hand OA in particular runs strongly in families.
Previous injuries: Torn meniscus, ACL injuries, fractures involving joints—these dramatically increase OA risk in the affected joint 10-20 years later. Post-traumatic arthritis is increasingly common with youth sports injuries.
Metabolic factors: Diabetes, metabolic syndrome, and chronic inflammation increase risk independent of weight. The systemic inflammation affects cartilage health.
The symptom pattern helps distinguish OA from other conditions:
Pain with use, better with rest (especially early on). Your knee hurts going down stairs but feels okay sitting. Hands ache after typing but not first thing in the morning.
Morning stiffness under 30 minutes. You feel stiff when you first wake up, but it improves as you move around. If stiffness lasts over an hour, that suggests inflammatory arthritis instead.
Crepitus—grinding, crunching, popping. Joint surfaces aren’t smooth anymore. You hear and feel them catching and grinding.
Reduced range of motion. The joint doesn’t fully extend or flex like it used to. This happens from cartilage loss, bone spurs, muscle tightness, and capsule changes.
Swelling after activity. The joint looks puffy after you’ve used it, particularly weight-bearing joints after walking or standing.
Instability or weakness. The joint feels unreliable, like it might give out. This comes from muscle weakness, ligament stretching, and altered mechanics.
X-rays show joint space narrowing (indicating cartilage loss you can’t see directly), bone spurs, and increased bone density in stressed areas. Early OA might not show on X-rays yet.
MRI reveals more—actual cartilage condition, meniscus tears, ligament issues, bone marrow changes. More expensive, usually reserved for surgical planning or unclear cases.
Physical examination by skilled practitioners reveals a lot—range of motion, crepitus, stability, pain patterns, muscle strength. Functional tests like single-leg balance or squat quality often predict impact better than imaging.
Blood tests rule out other conditions. OA doesn’t cause elevated inflammatory markers, unlike rheumatoid arthritis.
Weight loss (if relevant) is the most effective intervention for knee and hip OA. Even 10-15 pounds makes measurable differences in pain and function.
Appropriate exercise—walking, strength training, mobility work—slows progression and reduces pain. Immobility accelerates decline.
Targeted strengthening — especially for the knees — plays a major role in reducing pain and improving function, which is why specific knee exercises are often recommended for osteoarthritis management.
Anti-inflammatory diet and supplements—omega-3s, curcumin, Mediterranean eating patterns—manage the inflammatory component.
Natural anti-inflammatory compounds like curcumin have been studied for their role in supporting joint comfort and managing chronic inflammation.
Physical therapy for movement retraining, strength building, and pain management.
Medications when needed—NSAIDs occasionally, not daily if avoidable. Topical NSAIDs for hands with fewer systemic effects.
Joint replacement when conservative approaches fail and quality of life is significantly impaired. Highly successful for hips and knees when timing is right.
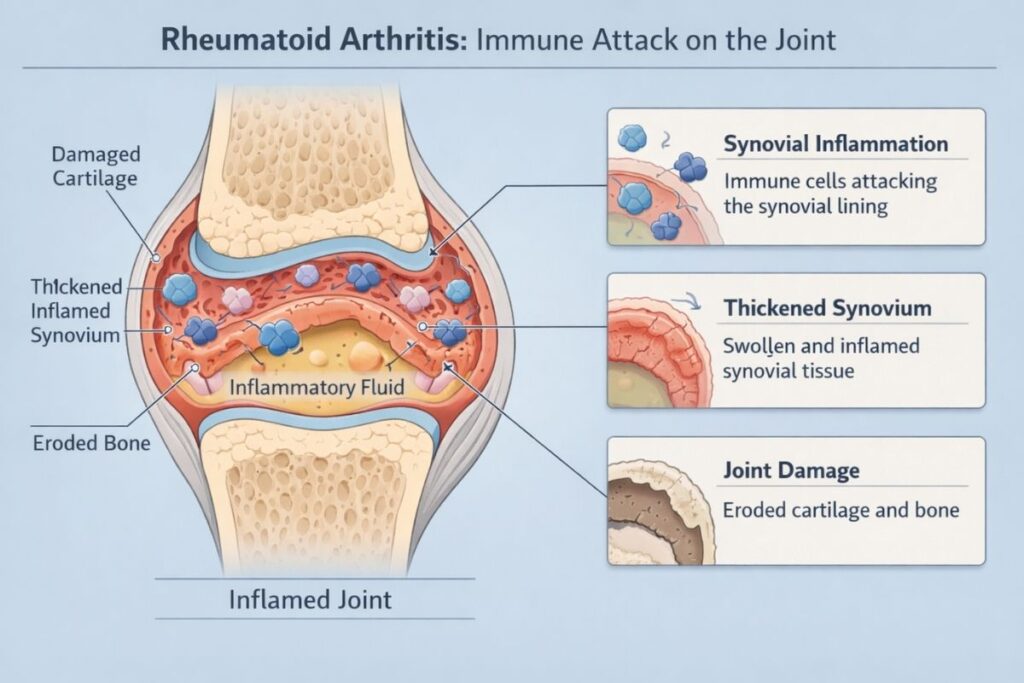
Rheumatoid arthritis is fundamentally different from osteoarthritis—it’s your immune system attacking your joints.
It’s basically a systemic autoimmune disease that requires early diagnosis and treatment to prevent permanent joint damage.
In RA, your immune system mistakes the synovial membrane lining your joints for a threat and attacks it. This creates severe inflammation that damages not just cartilage but the entire joint structure—ligaments, tendons, bones.
The inflammation is aggressive, destructive, and systemic. Unlike OA, RA causes symptoms throughout your body—fatigue, low-grade fever, malaise. It affects multiple joints symmetrically—both hands, both feet, both wrists.
Untreated, RA can cause permanent joint damage within months to years. Early aggressive treatment is critical to prevent irreversible destruction.
RA’s exact cause remains unclear, but several factors contribute:
Genetic susceptibility: Certain genes (particularly HLA types) increase risk. Having a first-degree relative with RA increases your risk significantly.
Environmental triggers: Smoking is the strongest modifiable risk factor. Infections, stress, and other environmental factors may trigger onset in genetically susceptible people.
Hormonal factors: RA affects women three times more than men. Onset often occurs after pregnancy or during perimenopause, suggesting hormonal influences.
Gut microbiome: Emerging research links gut bacteria composition to RA development and severity. Gut health interventions show promise in some studies.
Symmetrical joint pain and swelling. Both hands, both feet, both knees affected similarly. This symmetry is characteristic.
Morning stiffness lasting over an hour. You wake up feeling like you’re encased in cement. Movement gradually loosens you up, but it takes time.
Systemic symptoms: Fatigue, low-grade fever, general malaise. You feel sick beyond just joint pain.
Small joints affected first: Typically starts in hands and feet, particularly the small joints of fingers and toes. Can progress to larger joints.
Rheumatoid nodules: Firm lumps under skin, often on elbows or hands.
Flares and remissions: Symptoms wax and wane. Some days are manageable, others debilitating.
Blood tests are critical:
Imaging:
Clinical criteria: Doctors use scoring systems considering joint involvement, blood test results, symptom duration, and inflammatory markers.
Disease-modifying antirheumatic drugs (DMARDs) are the foundation. Methotrexate is typically first-line. These slow or halt joint damage progression.
Biologic agents for more aggressive disease or inadequate DMARD response. These target specific inflammatory pathways.
NSAIDs and corticosteroids manage symptoms but don’t prevent progression. Used alongside DMARDs.
Physical therapy maintains function and prevents deformities.
Lifestyle factors: Anti-inflammatory diet, smoking cessation, stress management, adequate sleep all influence disease activity.
Early aggressive treatment prevents irreversible damage. The “window of opportunity” in early RA makes prompt diagnosis and treatment critical.
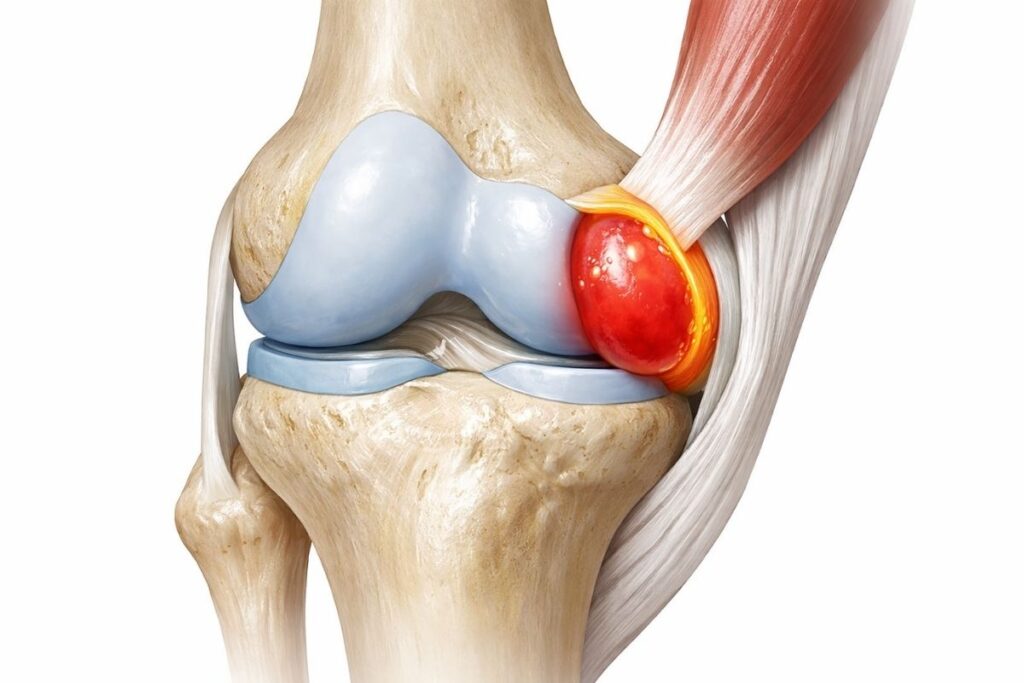
Bursae are small fluid-filled sacs cushioning areas where tendons or muscles glide over bones. When they get inflamed, it’s called bursitis.
Hip bursitis (trochanteric bursitis): Pain on the outside of your hip, worse lying on that side or climbing stairs. Often from tight IT bands, weak glutes, or repetitive stress.
Shoulder bursitis (subacromial bursitis): Pain with overhead reaching, often accompanied by rotator cuff issues. Impingement between the rotator cuff and the acromion irritates the bursa.
Knee bursitis: Several bursae around the knee can become inflamed. Prepatellar bursitis (in front of kneecap) from kneeling. Pes anserine bursitis (inner knee below joint line) often in people with OA or obesity.
Elbow bursitis: Swelling at the point of the elbow, sometimes from leaning on hard surfaces repeatedly.
Repetitive stress: Repeated movements irritating the bursa. Runners with hip bursitis from IT band friction. Painters with shoulder bursitis from overhead work.
Direct trauma: Falling on your hip or elbow. Kneeling on hard surfaces.
Underlying conditions: Bursitis commonly accompanies osteoarthritis, rheumatoid arthritis, gout, or infections (septic bursitis).
Biomechanical issues: Muscle tightness, weakness, or misalignments create abnormal stress on bursae.
Localized pain worse with specific movements or positions. Hip bursitis hurts lying on that side or with stairs. Shoulder bursitis hurts reaching overhead.
Point tenderness right over the affected bursa.
Swelling sometimes visible, particularly in elbow or knee bursitis.
No systemic symptoms unless infected. Septic bursitis causes fever, redness, warmth, and needs urgent medical attention.
Rest from aggravating activities (not complete immobility—just avoid what directly irritates it).
Ice reduces inflammation in acute phase.
NSAIDs for pain and inflammation management.
Physical therapy to address underlying biomechanical issues—tight IT band, weak glutes, shoulder impingement patterns.
Corticosteroid injections for severe or persistent cases.
Address root causes: Hip bursitis often won’t resolve until you address IT band tightness and glute weakness. Shoulder bursitis requires improving shoulder mechanics.
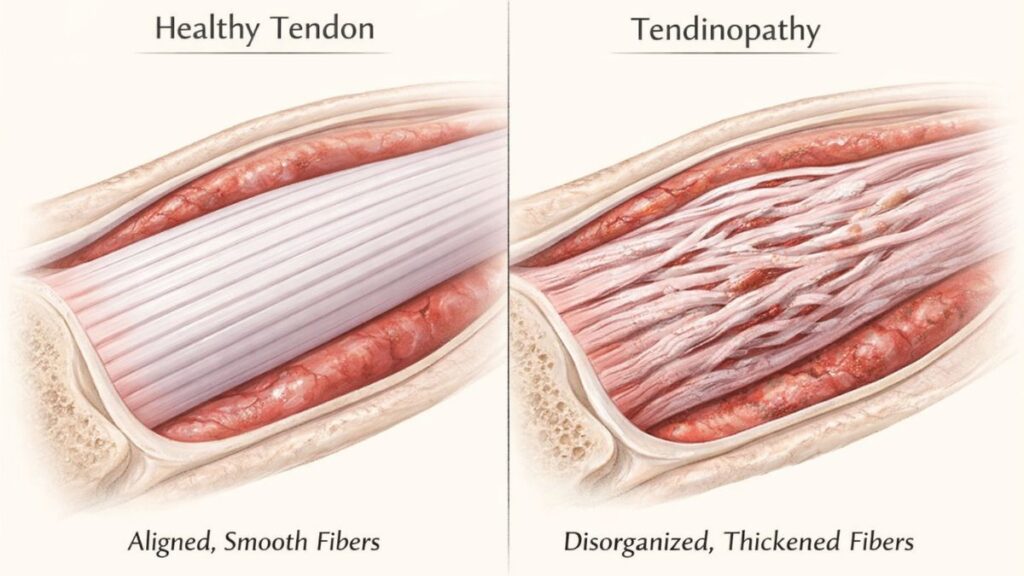
Tendons connect muscle to bone. When they’re irritated, inflamed, or degenerating, you get tendonitis or tendinopathy.
Tennis elbow (lateral epicondylitis): Outside elbow pain from gripping and wrist extension. Not just from tennis—any repetitive gripping.
Golfer’s elbow (medial epicondylitis): Inner elbow pain from wrist flexion and gripping.
Achilles tendonitis: Back of heel pain, particularly with running or jumping. Can progress to tendinopathy with degeneration if not addressed.
Patellar tendonitis (jumper’s knee): Front of knee below kneecap. Common in jumping sports.
Rotator cuff tendonitis: Shoulder pain with overhead activities, often progressing to impingement or tears if chronic.
Tendonitis implies acute inflammation. The tendon is irritated, inflamed, swollen. This is early-stage, often from sudden overuse.
Tendinopathy is chronic degeneration. The tendon structure breaks down, losing organization and strength. Less inflammation, more structural damage. Requires different treatment approach.
Many chronic “tendonitis” cases are actually tendinopathy—which is why rest and anti-inflammatories alone don’t fix them.
Overuse: Repetitive movements exceeding the tendon’s capacity to recover. Running too much too fast. Excessive typing or gripping.
Poor mechanics: Abnormal movement patterns load tendons incorrectly. Shoulder impingement creates rotator cuff problems. Poor running form stresses Achilles.
Sudden increases in activity: Going from sedentary to intense training. Tendons adapt slowly; muscles adapt faster. The strength imbalance stresses tendons.
Age: Tendons lose vascularity and healing capacity with age. Tendinopathy becomes more common after 40.
Previous injuries: Old sprains or strains that never fully healed properly.
Early (inflammatory) stage:
Research shows that eccentric loading exercises are one of the most effective treatments for chronic tendinopathy.
Chronic tendinopathy stage:
What doesn’t work: Rest alone rarely fixes chronic tendinopathy. The tendon needs appropriate loading to remodel and strengthen.
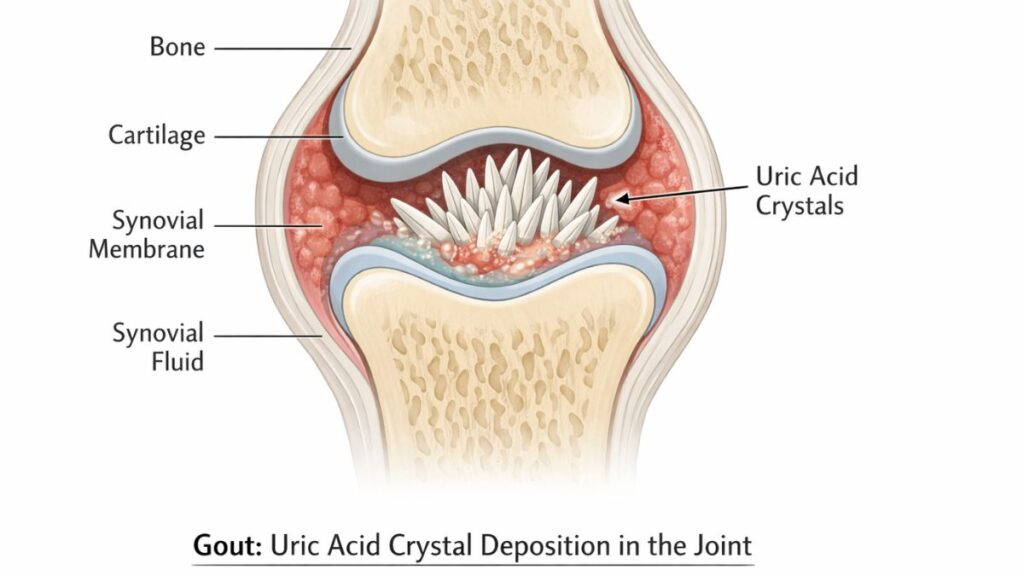
Gout is a specific type of inflammatory arthritis caused by uric acid crystals forming in joints.
When uric acid levels in your blood get too high (hyperuricemia), needle-sharp uric acid crystals can form in joints. Your immune system attacks these crystals, creating intense inflammation.
The classic presentation is sudden, severe pain in the big toe, but any joint can be affected.
Diet high in purines: Red meat, organ meats, certain seafood, alcohol (especially beer) increase uric acid.
Kidney issues: Kidneys not efficiently clearing uric acid. This can be genetic or from kidney disease.
Medications: Diuretics, aspirin, and some other drugs increase uric acid.
Dehydration: Concentrates uric acid in blood.
Metabolic syndrome: Obesity, high blood pressure, diabetes all increase gout risk.
Genetics: Strong hereditary component. If your parents had gout, your risk is much higher.
Sudden, severe pain typically overnight. You go to bed fine, wake up with excruciating pain.
Big toe most common but ankles, knees, fingers can be affected.
Joint is red, hot, swollen and exquisitely tender. Even a sheet touching it hurts.
Attacks last days to weeks then completely resolve. Between attacks, you feel fine.
Recurrent attacks if not treated. Frequency often increases over time.
Blood test showing elevated uric acid supports diagnosis, but normal uric acid during an attack doesn’t rule out gout.
Joint fluid analysis is definitive—extracting fluid and examining under microscope for uric acid crystals.
Imaging can show uric acid deposits (tophi) in chronic gout.
Acute attacks:
Long-term prevention:
Don’t start urate-lowering drugs during acute attack—can temporarily worsen symptoms. Start during remission periods.
Knowing which condition you’re dealing with changes everything about treatment approach.
Osteoarthritis vs Rheumatoid Arthritis:
Tendonitis vs Bursitis:
Gout vs Other Arthritis:
Inflammatory vs Mechanical:
Immediate medical attention for:
Prompt evaluation for:
Early intervention matters: Conditions like RA cause irreversible damage if not treated early. Don’t wait months to get evaluated.
Certain joint symptoms require prompt medical evaluation to rule out serious underlying conditions.
Understanding your specific condition gives you power to manage it effectively.
Educate yourself thoroughly. Read credible sources, understand your condition’s natural history, know what influences it. Knowledge reduces anxiety and improves outcomes.
Work with your healthcare team. Rheumatologists for RA, orthopedists for structural issues, physical therapists for rehabilitation, primary care for overall management.
Track your symptoms. What makes them better or worse? Patterns over time? This information guides treatment adjustments.
Be proactive, not passive. These conditions require active management—exercise, diet, weight management, medication adherence. Waiting for doctors to “fix” you rarely works.
Address mental health. Chronic pain and physical limitation affect mood and mental health. Depression and anxiety worsen pain perception. Mental health support is part of comprehensive care.
Connect with others. Support groups, online communities—talking with people managing the same condition provides practical insights and emotional support doctors can’t offer.
Maintain hope with realism. Many joint conditions are manageable but not curable. The goal is maintaining function and quality of life, not necessarily eliminating all symptoms. That’s a realistic, achievable target.
Regardless of diagnosis, long-term joint outcomes improve significantly when foundational joint health habits are applied consistently over time.
Your diagnosis isn’t a death sentence for your active life. It’s information that lets you adapt your approach intelligently. Understanding what’s actually wrong gives you the foundation to manage it effectively.
Note: This is educational information, not medical advice. Always work with qualified healthcare providers for diagnosis and treatment of joint conditions. Individual situations vary significantly.





