Physical Address
8206 Louisiana Blvd NE, Suite A N03815
Albuquerque, NM 87113
United States
Physical Address
8206 Louisiana Blvd NE, Suite A N03815
Albuquerque, NM 87113
United States

Your knees hurt, and someone told you to exercise them. The advice sounds backwards, right? But here's the reality: for most knee pain that isn't from acute injury or severe structural damage, the right exercises are the single most effective thing you can do. I'm not giving you twenty exercises hoping something sticks. I'm giving you five that actually matter—movements I've seen work for enough people over enough time that I can say with confidence: do these consistently, and your knees will likely feel better and function better.
Your knees hurt, and someone told you to exercise them. Maybe a doctor, maybe a physical therapist, maybe that friend who’s really into fitness. And now you’re here, probably skeptical, wondering how moving something that already hurts is supposed to help.
I get it. The advice sounds backwards.
But here’s the reality: for most knee pain that isn’t from acute injury or severe structural damage, the right exercises are probably the single most effective thing you can do. Not supplements, not braces, not rest. Movement.
I’m not going to give you twenty exercises and hope something sticks. I’m giving you five that actually matter, that I’ve seen work for enough people over enough time that I can say with confidence: if you do these consistently, your knees will likely feel better and function better. Not overnight, but genuinely better.
These aren’t random picks. They’re exercises that strengthen the muscles supporting your knees, improve stability, address common imbalances, and can be modified for almost any fitness level. Whether you’re dealing with osteoarthritis, patellofemoral pain, post-injury weakness, or just knees that feel unreliable, these movements form a solid foundation.
Let’s get into it.
Before we talk about specific exercises, you need to understand why this works.
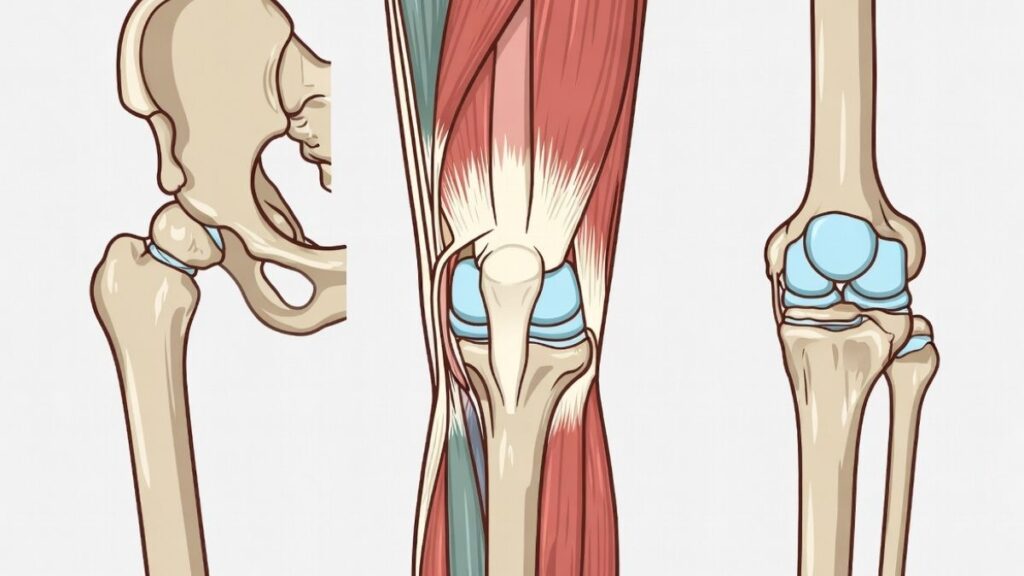
Your knee is basically a hinge joint caught between two much more complex joints—your hip above and your ankle below. It doesn’t have a ton of inherent stability on its own. What keeps it stable and functioning properly is the muscles around it, particularly your quadriceps, hamstrings, and glutes.
This relationship between muscle strength and knee joint loading is well documented in rehabilitation research. Clinical reviews published in sports medicine and physical therapy literature consistently show that stronger surrounding muscles reduce stress on cartilage and passive structures.
When those muscles are weak or imbalanced, your knee has to absorb forces it wasn’t designed to handle. The cartilage takes more stress. The ligaments work overtime. Small misalignments compound into bigger problems. Over time, this leads to pain, inflammation, and degeneration.
Strong muscles, on the other hand, act like shock absorbers and stabilizers. They distribute force more evenly, keep your knee tracking properly, and reduce the load on passive structures like cartilage and ligaments. This is why two people with the same degree of arthritis on an X-ray can have completely different pain levels—muscle strength makes an enormous difference.
Here’s what most people get wrong: they think rest will help their knees recover. Sometimes it does, especially after acute injury. But prolonged rest leads to muscle atrophy, which makes everything worse when you finally do start moving again. Your muscles got weaker while you were trying to protect your knees, and now your knees have even less support.
Public health guidance from the UK National Health Service (NHS) explicitly warns that avoiding movement for joint pain often leads to increased stiffness and weakness rather than recovery.
The solution isn’t to hammer your knees with high-impact activity they can’t handle. It’s to progressively strengthen the muscles around them with exercises that don’t aggravate the joint itself. That’s the balance we’re looking for.
This is where I start almost everyone, and for good reason.
Terminal knee extensions target the VMO—the teardrop-shaped muscle on the inner part of your quad just above your knee. This muscle is crucial for knee stability and proper tracking of your kneecap, and it tends to be weak or poorly activated in people with knee pain.
Here’s how you do it: Loop a resistance band around something sturdy at knee height—a table leg, a door anchor, whatever works. Step into the band so it’s behind your knee, and walk back until there’s tension. Start with your knee slightly bent (maybe 20-30 degrees). Now, straighten your knee fully against the band’s resistance, hold for a second, and return to the starting position.
That last bit of extension—the “terminal” part—is what really activates the VMO. Most people don’t fully straighten their knees in daily life, so this muscle doesn’t get worked properly. This exercise fixes that.
Start with light resistance. You should feel your quad working, especially that inner portion, but it shouldn’t hurt your knee. If it does, reduce the resistance or the range of motion. Do 15-20 reps, rest, repeat for 2-3 sets.
Why I like this exercise so much: it’s low-impact, easy to modify, hard to do wrong, and directly addresses one of the most common weak points in people with knee issues. It’s also something you can do daily without beating yourself up.
I’ve seen people with patellofemoral pain syndrome—that vague front-knee pain that’s hard to pin down—get significant relief just from doing terminal knee extensions consistently for a few weeks. It’s not flashy, but it works.

If terminal knee extensions are about isolation and control, step-downs are about functional strength and stability. This is where you start teaching your knee to handle real-world demands.
Find a step or a stable platform, anywhere from 4 to 8 inches high to start. Stand on it with one leg, the other leg hanging off the edge. Now, slowly lower your hanging foot toward the ground by bending your standing knee. Tap your heel lightly on the ground, then push back up to the starting position.
The key word here is slowly. This isn’t a cardio exercise. You’re controlling the descent, keeping your knee stable and aligned over your foot, not letting it cave inward. The eccentric phase—lowering down—is where a lot of the strength-building happens.
Watch your knee as you do this. If it wobbles side to side, or if it dives inward toward your midline, that’s a sign of weakness or poor motor control. Don’t panic, just work on it. Start with a lower step, use a wall or railing for light support, and focus on control over depth.
Aim for 10-12 reps per leg, 2-3 sets. If you can’t do that many with good form, do fewer. Quality matters infinitely more than quantity here.
Step-downs are brilliant because they mimic activities you do every day—going down stairs, stepping off curbs, getting out of a car. Strengthening this pattern carries over directly into real life. And because you’re working one leg at a time, you can’t compensate with your stronger side. Each leg has to do its own work.
I’ve had people tell me their knee pain going downstairs disappeared after a few weeks of step-downs. That’s not coincidence. You’re literally training the exact movement that was causing problems, making it stronger and more stable.

Your glutes might seem unrelated to your knees, but they’re absolutely critical.
Weak glutes—especially the gluteus medius—lead to poor hip stability, which causes your knee to track improperly and take on stress it shouldn’t. This is particularly common in runners and people with patellofemoral pain, but it shows up everywhere.
This hip–knee relationship is widely recognized in clinical biomechanics. The Mayo Clinic, for example, highlights hip and glute strength as a key factor in reducing knee strain and improving lower-body alignment.
Glute bridges are simple. Lie on your back, knees bent, feet flat on the floor about hip-width apart. Press through your heels and lift your hips up until your body forms a straight line from knees to shoulders. Squeeze your glutes at the top, hold for a second or two, then lower back down.
Don’t arch your lower back excessively—the movement should come from your hips, not your spine. And really focus on feeling your glutes doing the work, not your hamstrings or lower back. If you’re not sure, put your hands on your glutes as you lift. You should feel them contracting hard.
Do 15-20 reps, 2-3 sets. Once this feels easy, you can progress to single-leg glute bridges, which are significantly harder and more effective.
Here’s why this matters for your knees: when you walk, run, or go up stairs, your glutes stabilize your pelvis and control hip rotation. If they’re weak, your femur (thigh bone) rotates inward, which pulls your kneecap out of alignment and increases pressure on certain parts of your knee joint. Strengthen your glutes, and suddenly your knee tracks better without you consciously thinking about it.
I can’t tell you how many people I’ve talked to who were shocked that working their butt helped their knees. But it does, consistently and predictably.
Wall sits have a reputation for being boring and brutal. They’re both. They’re also incredibly effective for building isometric quad strength and knee stability.
Stand with your back against a wall, feet about hip-width apart and a foot or two away from the wall. Slide down until your knees are bent at roughly 90 degrees—like you’re sitting in an invisible chair. Your knees should be directly over your ankles, not pushing forward past your toes. Hold this position.
Start with 20-30 seconds if you’re new to this. Work up to 60 seconds or more. Rest, then repeat for 2-3 sets.
It’s going to burn. Your quads are going to fatigue. That’s the point. Isometric holds build endurance and strength in a way that dynamic exercises don’t quite replicate, and knee stability requires endurance—your muscles need to support your joints for extended periods, not just in quick bursts.
If 90 degrees is too intense, start higher. Even a partial squat against the wall builds strength. As you get stronger, you can go deeper, or add resistance by holding a weight.
One thing I really like about wall sits: they’re self-limiting. You can only hold them as long as your muscles can handle, so you’re unlikely to overdo it and hurt yourself. And they require zero equipment beyond a wall.
For people recovering from knee injuries or surgery, wall sits are often one of the first exercises physical therapists prescribe because they load the knee joint minimally while still building significant strength. That’s a useful combination.
This one targets the gluteus medius specifically, which is crucial for hip and knee stability.
Lie on your side with your knees bent at about 45 degrees, feet together. Keeping your feet touching, lift your top knee up toward the ceiling, opening your legs like a clamshell. Don’t let your hips roll backward—keep them stacked. Lower back down with control.
You can do this with just bodyweight, or add a resistance band around your thighs just above your knees for extra difficulty.
Do 15-20 reps per side, 2-3 sets.
Why does this matter? The gluteus medius controls hip abduction and prevents your knee from caving inward during single-leg activities. Weakness here is one of the biggest contributors to knee valgus—that inward collapse of the knee that increases injury risk and accelerates wear and tear.
Clamshells are deceptively hard if you do them correctly. A lot of people think they’re too easy because they’re using momentum or letting their hips rotate instead of isolating the glute. Focus on the muscle contraction. If you’re not feeling a burn in the side of your hip after 10-12 reps, you’re probably not doing them right.
I’ve seen runners eliminate knee pain just by adding clamshells and glute bridges to their routine a few times a week. The improvement in hip stability translates directly to better knee mechanics during running.
You now have five exercises. They’re good exercises. But exercises don’t work if you don’t do them, and most people don’t stick with exercise routines.
Here’s my advice: start with three days a week. Not seven. Not every day. Three days, ideally with a rest day in between. Monday, Wednesday, Friday. Tuesday, Thursday, Saturday. Whatever fits your life.
Do all five exercises in sequence. It’ll take you maybe 15-20 minutes once you get the hang of it. That’s manageable. That’s sustainable.
Don’t go hard out of the gate. Start with lighter resistance, fewer reps, whatever you can handle without significant pain during or after. The goal in the first two weeks is consistency and learning the movements, not maxing out your effort.
Pay attention to how your knees feel the next day. Some muscle soreness is fine—that’s normal. But if your knee pain gets worse or you develop new sharp pains, back off. Reduce intensity, check your form, maybe skip one exercise and see if that helps. Pain during the exercise is a signal to modify, not push through.
And here’s the hardest part: you need to do this for weeks before you decide if it’s working. Not days, weeks. Muscle adaptation takes time. Most people start noticing improvements around the 3-4 week mark if they’re consistent. Some sooner, some later.
If after six weeks of honest, consistent effort you’re not seeing any improvement—or if things are getting worse—it’s worth seeing a professional. These exercises work for most common knee issues, but not everything. Sometimes you need a proper diagnosis and individualized treatment.
Once the exercises feel easy, you need to progress them. Your muscles adapt, and if you keep doing the same thing at the same intensity forever, you’ll plateau.
For terminal knee extensions, use a heavier resistance band. For step-downs, increase the height of the step or add weight. For glute bridges, progress to single-leg variations. For wall sits, go deeper or hold longer. For clamshells, add a resistance band.
Progression doesn’t mean making things harder for the sake of it. It means continuing to challenge your muscles so they keep getting stronger. Once you can comfortably do 20 reps of something with good form, it’s probably time to make it a bit harder.
But don’t rush this. Weeks or months of gradual progression will get you much further than trying to jump to advanced variations before you’re ready.
I need to be clear about limitations.
These exercises won’t repair a torn meniscus or ACL. They won’t reverse severe arthritis where cartilage is completely gone. They won’t fix mechanical issues that require surgical intervention.
What they will do is strengthen the muscles around your knee, improve stability, reduce compensatory stress on the joint, and often significantly reduce pain and improve function for issues that are muscular or alignment-related.
If you have severe swelling, sharp pain that doesn’t improve with rest, locking or catching sensations, or instability where your knee gives out, you need to see a doctor before starting any exercise program. These exercises are fantastic for common knee pain and weakness, but they’re not a substitute for proper medical evaluation when needed.
Knee health isn’t just about these five exercises. It’s also about maintaining a healthy weight if that’s relevant to your situation, staying generally active, avoiding prolonged inactivity, wearing appropriate footwear, and not ignoring early warning signs of problems.
But if I had to choose one intervention that gives the most return for the least investment, it’s strengthening exercises. Nothing else comes close.
You can spend hundreds on supplements, braces, and gadgets. Or you can spend 15 minutes three times a week doing movements that actually address the root cause of most knee pain—muscle weakness and instability.
These exercises fit into a broader approach to active aging after 50, where strength, mobility, and consistency are what keep joints functional long-term.
Your knees support you through everything you do. Taking care of them isn’t complicated, but it does require consistency and a bit of patience.
These five exercises are a solid place to start.
Note: This is information based on research and experience, not medical advice. If you have significant knee pain, injury, or medical conditions, consult with a healthcare provider or physical therapist before starting new exercises. They can assess your specific situation and provide personalized guidance.






